
Receiving a diagnosis of congenital diaphragmatic hernia (CDH), whether during a routine prenatal ultrasound or immediately after your baby is born, is an overwhelming experience. The unfamiliar medical terminology, the urgency of the situation, and the uncertainty about what comes next can leave parents feeling lost.
This guide is written to change that. Dr. Deepak Subramanian and the team at Chennai Hernia Care believe that informed parents are better equipped to support their child’s care, ask the right questions, and make confident decisions alongside their medical team.
Here, we explain what CDH is, the three primary types, how each is diagnosed, and what treatment typically involves, in an understandable way, without sacrificing medical accuracy.
What Is Congenital Diaphragmatic Hernia?
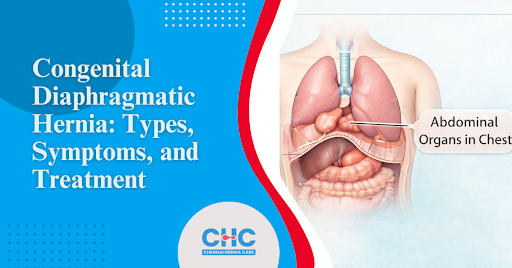
The diaphragm is a dome-shaped muscle that separates the chest cavity (which contains the heart and lungs) from the abdominal cavity (which contains the stomach, intestines, and liver). It plays a central role in breathing by contracting and relaxing with every breath.
In a congenital diaphragmatic hernia, the diaphragm does not form completely during fetal development, leaving an abnormal opening or defect. During pregnancy, through this gap, abdominal organs migrate upward into the chest cavity, where they compete with the developing lungs for space. This crowding is what makes CDH a serious condition: it can prevent the lungs from developing fully, a complication known as pulmonary hypoplasia (underdeveloped lungs).
CDH occurs in approximately 1 in every 2,500 live births, according to the National Institutes of Health (NIH). It is not caused by anything the mother did during pregnancy it arises from a disruption in fetal development, typically between the 8th and 10th week of gestation (the early weeks of pregnancy when organs are forming).
To understand how congenital hernias differ from hernias that develop later in life, visit Congenital Hernia: Causes, Types, and Treatment
The Three Primary Types of Congenital Diaphragmatic Hernia
CDH is not a single uniform condition. Its clinical behavior, severity, and surgical approach vary significantly depending on where on the diaphragm the defect occurs.
1. Bochdalek Hernia — The Most Common Type
Bochdalek hernia accounts for approximately 85–90% of all CDH cases, making it by far the most frequently encountered type. The defect occurs in the posterolateral (back and side) portion of the diaphragm, most often on the left side, in around 80–85% of cases.
Because the defect is large and located at the back of the diaphragm, it creates an open pathway through which the stomach, small intestine, large intestine, spleen, and, in some cases, the left lobe of the liver herniate (push through) into the chest cavity. The left lung is typically the most severely compressed, though bilateral (both-sided) Bochdalek hernias — while rare — carry an extremely high mortality risk.
Why the left side is more commonly affected: During fetal development, the right side of the diaphragm closes slightly earlier than the left. This timing difference means the left side is more vulnerable to incomplete closure.
Clinical severity of Bochdalek hernia depends on two key factors:
- The size of the defect – larger defects allow more organs to herniate, causing greater lung compression
- The liver position – when the liver herniates into the chest (a condition called “liver up”), outcomes are generally more serious because liver herniation is associated with more severe pulmonary hypoplasia
Babies with Bochdalek hernia typically present at birth with respiratory distress (difficulty breathing), a barrel-shaped or asymmetrical chest, a concave (sunken) abdomen, and absent or diminished breath sounds on the affected side. These signs require immediate neonatal intensive care unit (NICU) stabilisation.
For a detailed clinical comparison of Bochdalek and Morgagni hernias, read Bochdalek Hernia vs Morgagni Hernia: Comprehensive Medical Insights
2. Morgagni Hernia – The Rarest Type
Morgagni hernia represents only 2–3% of CDH cases and is the least common of the three types. The defect is located at the anterior (front) and central portion of the diaphragm, specifically through a gap called the foramen of Morgagni, a small natural opening near the sternum (breastbone) that fails to close properly before birth.
Unlike Bochdalek hernia, Morgagni hernia is almost always right-sided, and the organs that most commonly herniate through this defect are the transverse colon (part of the large intestine) and omentum (a fatty tissue layer that covers the abdominal organs). The stomach, small bowel, and liver may also be involved in larger defects.
Because the defect is smaller and the herniated contents tend to be less critical than in Bochdalek hernia, Morgagni hernia is frequently asymptomatic at birth (showing no symptoms in the newborn period). Many cases are identified incidentally discovered during a chest X-ray or CT scan performed for another reason, sometimes in childhood or even adulthood.
When symptoms do appear, they are typically gastrointestinal (related to digestion) rather than respiratory, and may include:
- Recurrent chest infections
- Chronic cough
- Mild breathing difficulty
- Vomiting or feeding difficulties in infants
- Abdominal discomfort in older children or adults
Despite its generally milder presentation, surgical repair is still recommended once Morgagni hernia is identified to prevent the risk of bowel obstruction (a blockage in the intestine) or strangulation (where the blood supply to herniated tissue is cut off, requiring emergency surgery).
3. Central Diaphragmatic Hernia: The Most Complex Type
Central diaphragmatic hernia is the rarest and most surgically challenging form of CDH. As the name indicates, the defect occurs in the central tendon (the flat, fibrous central portion of the diaphragm), rather than at its muscular edges. This central location makes the defect structurally more difficult to repair and is often associated with other congenital anomalies (abnormalities present from birth).
Central CDH may occur in isolation or as part of broader syndromes such as Cantrell’s pentalogy — a rare complex of five associated birth defects involving the heart, abdominal wall, sternum, diaphragm, and pericardium (the sac surrounding the heart).
Surgical repair of a central diaphragmatic hernia is particularly complex because the defect often cannot be closed with the patient’s own diaphragmatic tissue alone. A prosthetic patch (a synthetic material used to reconstruct the diaphragm) or biological graft (tissue from another source) is frequently required to complete the repair, which increases the risk of recurrence as the child grows.
How Is CDH Diagnosed?
Prenatal diagnosis (diagnosis before birth) is now possible in the majority of CDH cases, thanks to routine obstetric ultrasound scanning. CDH is typically identified between 18 and 24 weeks of gestation when abdominal organs are visible in the chest cavity on ultrasound imaging.
Once CDH is suspected on ultrasound, additional imaging including fetal MRI (Magnetic Resonance Imaging, a detailed scan that does not use radiation) provides more precise information about the defect’s size, the degree of lung development, and whether the liver has herniated into the chest. These findings directly guide prognosis and delivery planning.
Two key measurements help predict severity before birth:
- Lung-to-Head Ratio (LHR): A calculation comparing the size of the baby’s remaining lung tissue to the size of the head. A lower LHR indicates more severe lung compression.
- Observed/Expected LHR (O/E LHR): A refined version of the above measurement, now considered the more reliable predictor of postnatal (after birth) outcome, according to The Lancet.
For babies diagnosed after birth, chest X-ray remains the primary confirmatory tool, showing bowel loops or other abdominal organs clearly visible within the chest cavity.
Learn about the broader spectrum of hernia types and how they are classified: What Are the Types of Hernias?
Treatment: What Happens After Diagnosis?
CDH treatment is always surgical there is no non-surgical resolution for a diaphragmatic defect. However, the timing and sequence of treatment are equally important as the surgery itself.
Immediate priority at birth is stabilisation, not surgery. Babies born with CDH, particularly Bochdalek type, require urgent NICU admission for respiratory support. This typically involves gentle ventilation (carefully controlled breathing support to avoid further lung injury), medications to reduce pulmonary hypertension (high blood pressure in the lung’s blood vessels, which is common in CDH), and in severe cases, ECMO (Extracorporeal Membrane Oxygenation, a machine that temporarily takes over the function of the heart and lungs to allow the body to stabilise).
Surgical repair is performed once the baby is medically stable, usually within the first few days of life, though timing varies by centre and clinical condition. The surgeon returns the herniated organs to the abdominal cavity and closes the diaphragmatic defect, using the baby’s own tissue where possible or a prosthetic patch for larger defects.
According to the British Journal of Surgery, survival rates for CDH have improved significantly over the past two decades, with outcomes strongly correlated to the degree of pulmonary hypoplasia and the presence of associated anomalies.
For guidance on what to expect in the recovery period after hernia surgery → Hernia Surgery Recovery Timeline: A Week-by-Week Guide
CDH and Long-Term Outcomes: What Parents Should Know
Surviving CDH is not the end of the journey. Many children require ongoing follow-up for:
- Pulmonary development lungs continue to grow after birth, and respiratory function often improves over the years
- Gastroesophageal reflux (stomach acid moving back up the oesophagus the food pipe), which is common after CDH repair
- Hernia recurrence is particularly problematic after patch repair, as the prosthetic material does not grow with the child
- Neurodevelopmental monitoring of children who require ECMO support is at higher risk for developmental delays and benefits from early intervention programs
The CDH International Foundation offers peer support, research updates, and resources specifically for CDH families navigating long-term care.
A Note for Parents
A CDH diagnosis changes everything in an instant. The weeks between prenatal diagnosis and delivery or the hours after birth can feel isolating and frightening. At Chennai Hernia Care, Dr. Deepak Subramanian understands that parents need clear information, honest answers, and a specialist they can trust.
If your baby has been diagnosed with CDH, or if you have questions about a hernia condition identified during pregnancy, we encourage you to reach out for a consultation.
Medically reviewed content. External references: National Institutes of Health – CDH | The Lancet – Fetal CDH Outcomes | British Journal of Surgery – CDH Survival | CDH International Foundation
Frequently Asked Questions (FAQs)
Bochdalek hernia is the most common, accounting for 85–90% of all CDH cases. It occurs at the back and side of the diaphragm, most often on the left side, and typically presents with significant respiratory distress at birth.
Yes. Most CDH cases are identified between 18 and 24 weeks of pregnancy through routine ultrasound. Fetal MRI provides additional detail to help assess severity and plan delivery and postnatal care.
Severity varies considerably. Bochdalek herniation, especially with liver herniation, carries a higher risk, while Morgagni hernia is often mild and discovered incidentally. Survival rates have improved significantly with advances in neonatal intensive care and surgical technique.
CDH results from incomplete closure of the diaphragm during fetal development, typically between weeks 8 and 10 of pregnancy. It is not caused by anything the mother did or did not do during pregnancy. In some cases, a genetic or chromosomal factor is identified, but many CDH cases occur without a known cause.
Recurrence is possible, particularly after patch repair in large defects. As the child grows, the prosthetic patch does not expand, which can create tension at the repair margins over time. Long-term surgical follow-up is essential.
Yes. Surgical repair is the only definitive treatment. The timing of surgery depends on the baby’s stability, immediate stabilisation and respiratory support always take priority over rushing to the operating room.
Our Medical Review Process:
Our content goes through a structured review process to ensure medical accuracy and reliability.
Written By: Editorial Team, Chennai Hernia Care
Reviewed By: Dr. Deepak Subramanian, MS, FMAS – Laparoscopic & Bariatric Surgeon
Last Updated: June 1, 2026
